
Search
- Page Path
- HOME > Search
Original Articles
- Thyroid
- Prognostic Roles of Inflammatory Biomarkers in Radioiodine-Refractory Thyroid Cancer Treated with Lenvatinib
- Chae A Kim, Mijin Kim, Meihua Jin, Hee Kyung Kim, Min Ji Jeon, Dong Jun Lim, Bo Hyun Kim, Ho-Cheol Kang, Won Bae Kim, Dong Yeob Shin, Won Gu Kim
- Endocrinol Metab. 2024;39(2):334-343. Published online April 4, 2024
- DOI: https://doi.org/10.3803/EnM.2023.1854
- 351 View
- 24 Download
-
 Abstract
Abstract
 PDF
PDF Supplementary Material
Supplementary Material PubReader
PubReader  ePub
ePub - Background
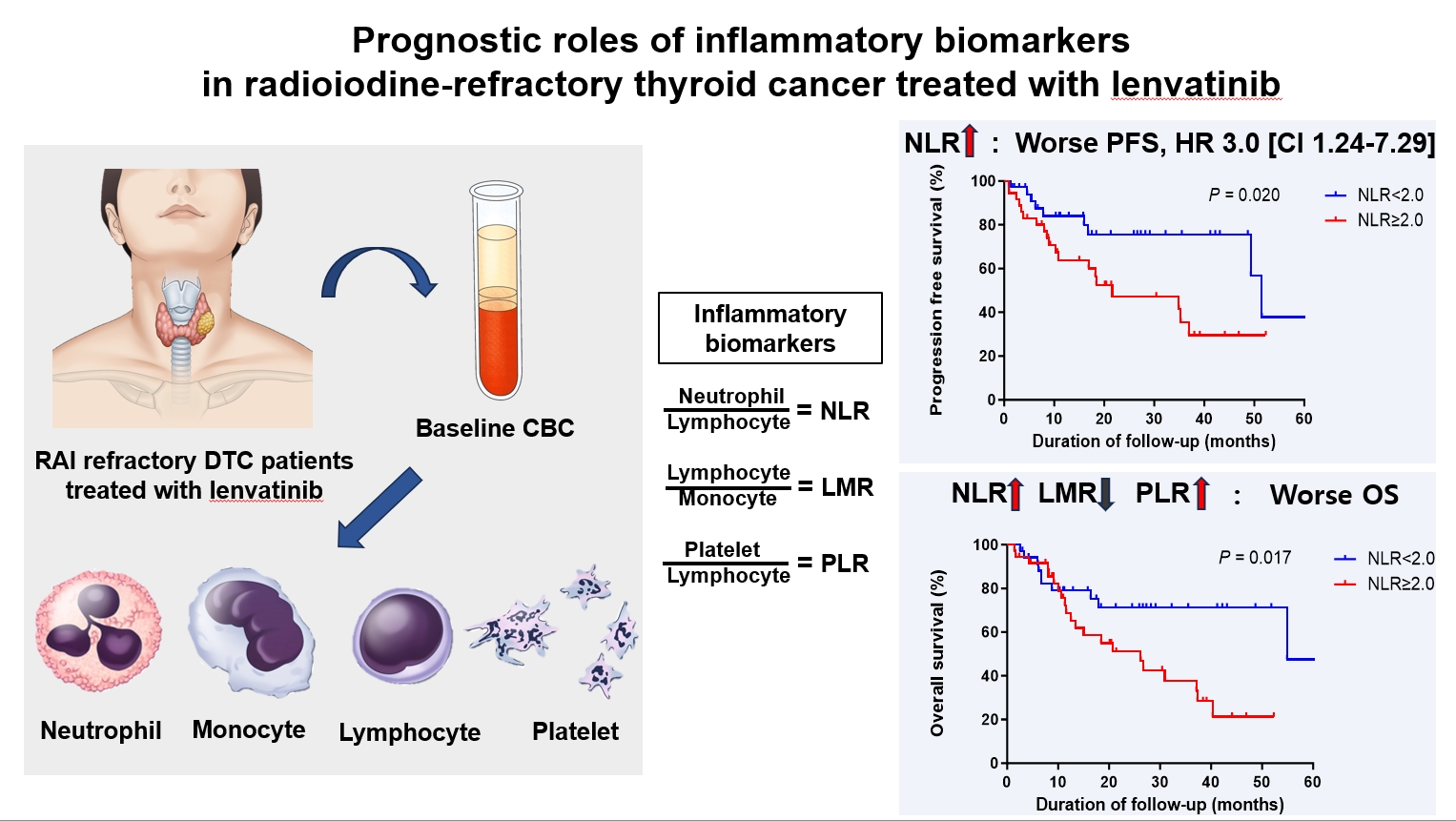
Inflammatory biomarkers, such as the neutrophil-to-lymphocyte ratio (NLR), lymphocyte-to-monocyte ratio (LMR), and platelet-to-lymphocyte ratio (PLR), serve as valuable prognostic indicators in various cancers. This multicenter, retrospective cohort study assessed the treatment outcomes of lenvatinib in 71 patients with radioactive iodine (RAI)-refractory thyroid cancer, considering the baseline inflammatory biomarkers.
Methods
This study retrospectively included patients from five tertiary hospitals in Korea whose complete blood counts were available before lenvatinib treatment. Progression-free survival (PFS) and overall survival (OS) were evaluated based on the median value of inflammatory biomarkers.
Results
No significant differences in baseline characteristics were observed among patients grouped according to the inflammatory biomarkers, except for older patients with a higher-than-median NLR (≥2) compared to their counterparts with a lower NLR (P= 0.01). Patients with a higher-than-median NLR had significantly shorter PFS (P=0.02) and OS (P=0.017) than those with a lower NLR. In multivariate analysis, a higher-than-median NLR was significantly associated with poor OS (hazard ratio, 3.0; 95% confidence interval, 1.24 to 7.29; P=0.015). However, neither the LMR nor the PLR was associated with PFS. A higher-than-median LMR (≥3.9) was significantly associated with prolonged OS compared to a lower LMR (P=0.036). In contrast, a higher-than-median PLR (≥142.1) was associated with shorter OS compared to a lower PLR (P=0.039).
Conclusion
Baseline inflammatory biomarkers can serve as predictive indicators of PFS and OS in patients with RAI-refractory thyroid cancer treated with lenvatinib.

- Thyroid
- Immunoglobulin G4-Related Thyroid Disease: A Single-Center Experience and Literature Review
- Meihua Jin, Bictdeun Kim, Ahreum Jang, Min Ji Jeon, Young Jun Choi, Yu-Mi Lee, Dong Eun Song, Won Gu Kim
- Endocrinol Metab. 2022;37(2):312-322. Published online April 25, 2022
- DOI: https://doi.org/10.3803/EnM.2021.1318
- 4,033 View
- 180 Download
- 2 Web of Science
- 2 Crossref
-
Abstract
PDFPubReader ePub
- Background
Immunoglobulin G4 (IgG4)-related disease is an entity that can involve the thyroid gland. The spectrum of IgG4-related thyroid disease (IgG4-RTD) includes Hashimoto thyroiditis (HT) and its fibrotic variant, Riedel thyroiditis, as well as Graves’ disease. The early diagnosis of IgG4-RTD is important because it is a medically treatable disease, and a delay in the diagnosis might result in unnecessary surgery. We present a case series of IgG4-RTD with a review of the literature.
Methods
We retrospectively reviewed the clinical presentation and the radiological and pathological findings of patients diagnosed with IgG4-RTD between 2017 and 2021 at a tertiary medical center in Korea. We also conducted a literature review of IgG4-RTD.
Results
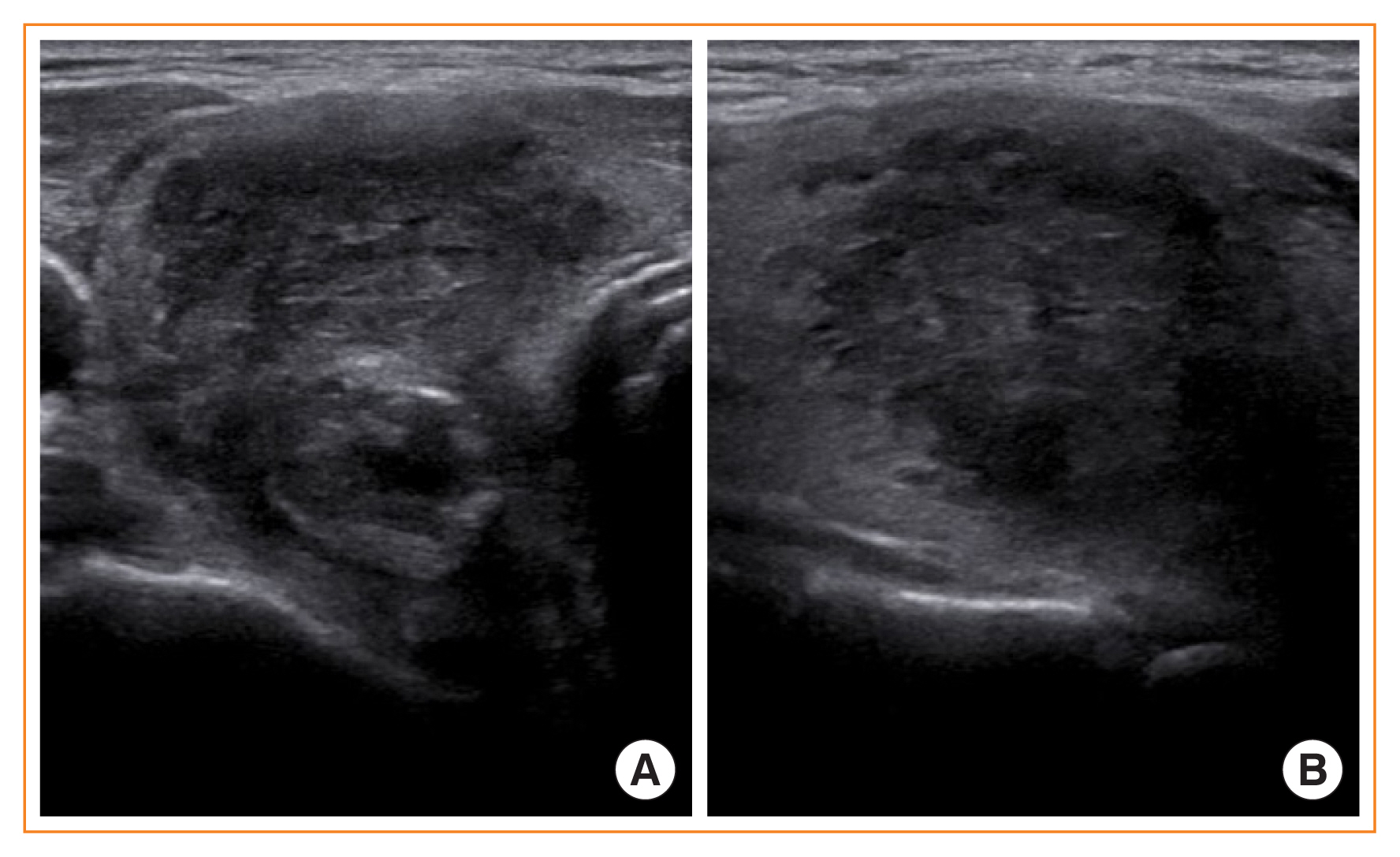
Five patients were diagnosed with IgG4-RTD during the study period. The patients’ age ranged from 31 to 76 years, and three patients were men. Most patients visited the clinic for a neck mass, and hypoechogenic nodular lesions were observed on neck ultrasonography. Three patients had IgG4 HT, and two patients had IgG4 Riedel thyroiditis. All patients developed hypothyroidism that necessitated L-thyroxine replacement. The diagnosis of IgG4-RTD was confirmed after a pathological examination of the surgical specimen in the first two cases. However, the early diagnosis was possible after a core needle biopsy in three clinically suspected patients.
Conclusion
The diagnosis of IgG4-RTD requires clinical suspicion combined with serology and histological analyses using IgG4 immunostaining. The early diagnosis of IgG4-RTD is difficult; thus, biopsy with IgG4 immunostaining and serum IgG4 measurements will help diagnose patients suspected of having IgG4-RTD. -
Citations
Citations to this article as recorded by
- Are sonographic characteristics of Hashimoto’s thyroiditis related with immunologic parameters? A cross-sectional study
K. Kenarlı, A. B. Bahçecioğlu, Ö. B. Aksu, S. Güllü
Journal of Endocrinological Investigation.2024;[Epub] CrossRef - Reshaping the Concept of Riedel’s Thyroiditis into the Larger Frame of IgG4-Related Disease (Spectrum of IgG4-Related Thyroid Disease)
Mara Carsote, Claudiu Nistor
Biomedicines.2023; 11(6): 1691. CrossRef
- Are sonographic characteristics of Hashimoto’s thyroiditis related with immunologic parameters? A cross-sectional study
- Thyroid
- Clinical Characteristics and Prognosis of Coexisting Thyroid Cancer in Patients with Graves’ Disease: A Retrospective Multicenter Study
- Jee Hee Yoon, Meihua Jin, Mijin Kim, A Ram Hong, Hee Kyung Kim, Bo Hyun Kim, Won Bae Kim, Young Kee Shong, Min Ji Jeon, Ho-Cheol Kang
- Endocrinol Metab. 2021;36(6):1268-1276. Published online November 26, 2021
- DOI: https://doi.org/10.3803/EnM.2021.1227
- 4,844 View
- 186 Download
- 10 Web of Science
- 11 Crossref
-
Abstract
PDFSupplementary MaterialPubReader ePub
- Background
The association between Graves’ disease (GD) and co-existing thyroid cancer is still controversial and most of the previously reported data have been based on surgically treated GD patients. This study investigated the clinicopathological findings and prognosis of concomitant thyroid cancer in GD patients in the era of widespread application of ultrasonography.
Methods
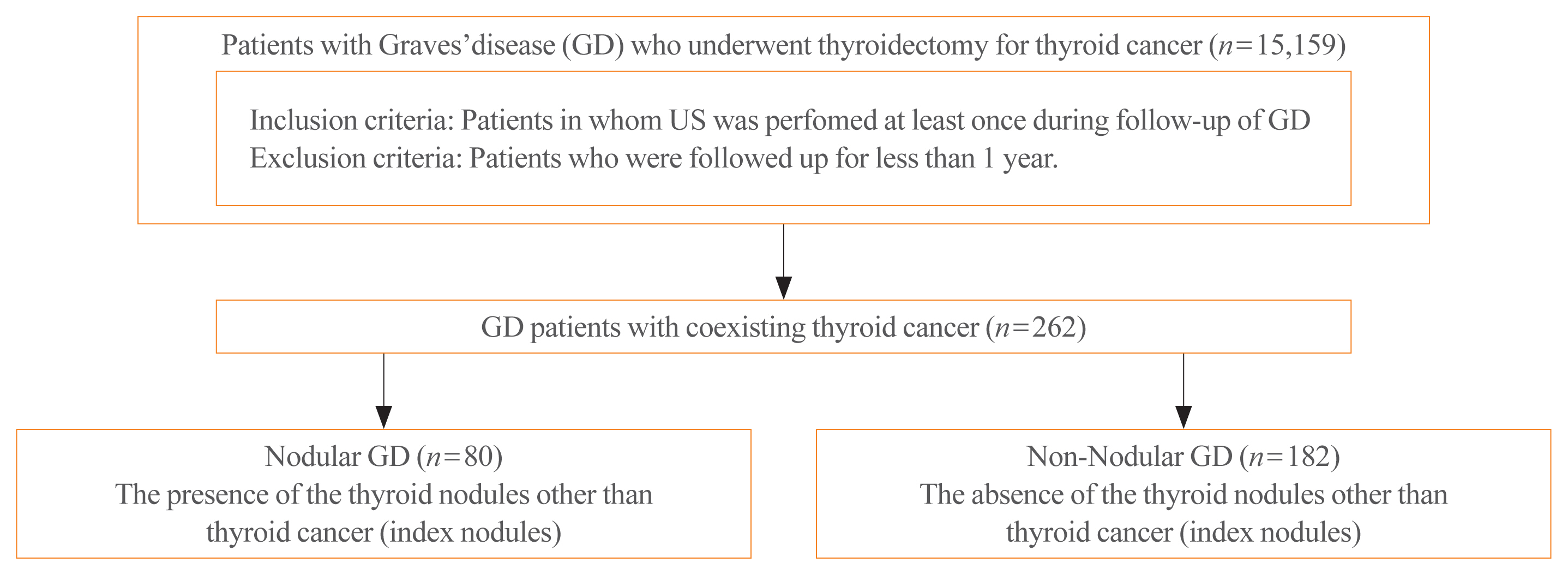
Data of GD patients who underwent thyroidectomy for thyroid cancer between 2010 and 2019 in three tertiary hospitals in South Korea (Asan Medical Center, Chonnam National University Hwasun Hospital, and Pusan National University Hospital) were collected and analyzed retrospectively. In the subgroup analysis, aggressiveness and clinical outcomes of thyroid cancer were compared nodular GD and non-nodular GD groups according to the presence or absence of the thyroid nodules other than thyroid cancer (index nodules).
Results
Of the 15,159 GD patients treated at the hospitals during the study period, 262 (1.7%) underwent thyroidectomy for coexisting thyroid cancer. Eleven patients (4.2%) were diagnosed with occult thyroid cancer and 182 patients (69.5%) had microcarcinomas. No differences in thyroid cancer aggressiveness, ultrasonographic findings, or prognosis were observed between the nodular GD and non-nodular GD groups except the cancer subtype. In the multivariate analysis, only lymph node (LN) metastasis was an independent prognostic factor for recurrent/persistent disease of thyroid cancer arising in GD (P=0.020).
Conclusion
The prevalence of concomitant thyroid cancer in GD patients was considerably lower than in previous reports. The clinical outcomes of thyroid cancer in GD patients were also excellent but, more cautious follow-up is necessary for patients with LN metastasis in the same way as for thyroid cancer in non-GD patients. -
Citations
Citations to this article as recorded by- Comparison of Surgical Outcomes of Transoral Versus Open Thyroidectomy for Graves Disease
Suo-Hsien Wang, Wu-Po Chao, Ta-You Lo, Soh-Ching Ng, Yu-Hsien Chen
Surgical Laparoscopy, Endoscopy & Percutaneous Techniques.2024; 34(2): 150. CrossRef - Outcomes of Surgical Treatment for Graves’ Disease: A Single-Center Experience of 216 Cases
Hanxing Sun, Hui Tong, Xiaohui Shen, Haoji Gao, Jie Kuang, Xi Chen, Qinyu Li, Weihua Qiu, Zhuoran Liu, Jiqi Yan
Journal of Clinical Medicine.2023; 12(4): 1308. CrossRef - Cancer and Mortality Risks of Graves’ Disease in South Korea Based on National Data from 2010 to 2019
Young Ju Choi, Kyungdo Han, Won Kyoung Cho, Min Ho Jung, Byung-Kyu Suh
Clinical Epidemiology.2023; Volume 15: 535. CrossRef - Risk and Prognosis of Thyroid Cancer in Patients with Graves’ Disease: An Umbrella Review
Marco Palella, Francesca Maria Giustolisi, Adriana Modica Fiascaro, Martina Fichera, Antonella Palmieri, Rossella Cannarella, Aldo E. Calogero, Margherita Ferrante, Maria Fiore
Cancers.2023; 15(10): 2724. CrossRef - Characteristics, staging and outcomes of differentiated thyroid cancer in patients with and without Graves’ disease
Chaitra Gopinath, Hanna Crow, Sujata Panthi, Leonidas Bantis, Kenneth D. Burman, Chitra Choudhary
Journal of Clinical & Translational Endocrinology.2023; 33: 100321. CrossRef - Prevalence, Treatment Status, and Comorbidities of Hyperthyroidism in Korea from 2003 to 2018: A Nationwide Population Study
Hwa Young Ahn, Sun Wook Cho, Mi Young Lee, Young Joo Park, Bon Seok Koo, Hang-Seok Chang, Ka Hee Yi
Endocrinology and Metabolism.2023; 38(4): 436. CrossRef - Hashimoto’s Thyroiditis and Papillary Thyroid Carcinoma: A Follow-Up Study in Patients with Absence of Aggressive Risk Factors at the Surgery of the Primary Tumor
Andrea Marongiu, Susanna Nuvoli, Andrea De Vito, Sonia Vargiu, Angela Spanu, Giuseppe Madeddu
Diagnostics.2023; 13(19): 3068. CrossRef - Table of Contents
Clinical Thyroidology.2022; 34(2): 48. CrossRef - Predisposition to and Prognosis of Thyroid Cancer May Not Be Affected by Graves’ Disease, But Some Questions Still Remain
Yanrui Huang, Haixia Guan
Clinical Thyroidology.2022; 34(2): 59. CrossRef - A Comparative Follow-Up Study of Patients with Papillary Thyroid Carcinoma Associated or Not with Graves’ Disease
Andrea Marongiu, Susanna Nuvoli, Andrea De Vito, Maria Rondini, Angela Spanu, Giuseppe Madeddu
Diagnostics.2022; 12(11): 2801. CrossRef - An unusual case of papillary thyroid carcinoma presenting as Graves’ disease
Pooja Tiwari, Uma Kaimal Saikia, Abhamoni Baro, Ashok Krishna Bhuyan
Thyroid Research and Practice.2022; 19(1): 47. CrossRef
- Comparison of Surgical Outcomes of Transoral Versus Open Thyroidectomy for Graves Disease
- Thyroid
- Clinicopathological Characteristics and Disease-Free Survival in Patients with Hürthle Cell Carcinoma: A Multicenter Cohort Study in South Korea
- Meihua Jin, Eun Sook Kim, Bo Hyun Kim, Hee Kyung Kim, Yea Eun Kang, Min Ji Jeon, Tae Yong Kim, Ho-Cheol Kang, Won Bae Kim, Young Kee Shong, Mijin Kim, Won Gu Kim
- Endocrinol Metab. 2021;36(5):1078-1085. Published online October 28, 2021
- DOI: https://doi.org/10.3803/EnM.2021.1151
- 3,892 View
- 110 Download
- 4 Web of Science
- 4 Crossref
-
Abstract
PDFSupplementary MaterialPubReader ePub
- Background
Hürthle cell carcinoma (HCC), a type of thyroid carcinoma, is rare in South Korea, and few studies have investigated its prognosis.
Methods
This long-term multicenter retrospective cohort study evaluated the clinicopathological features and clinical outcomes in patients with HCC who underwent thyroid surgery between 1996 and 2009.
Results
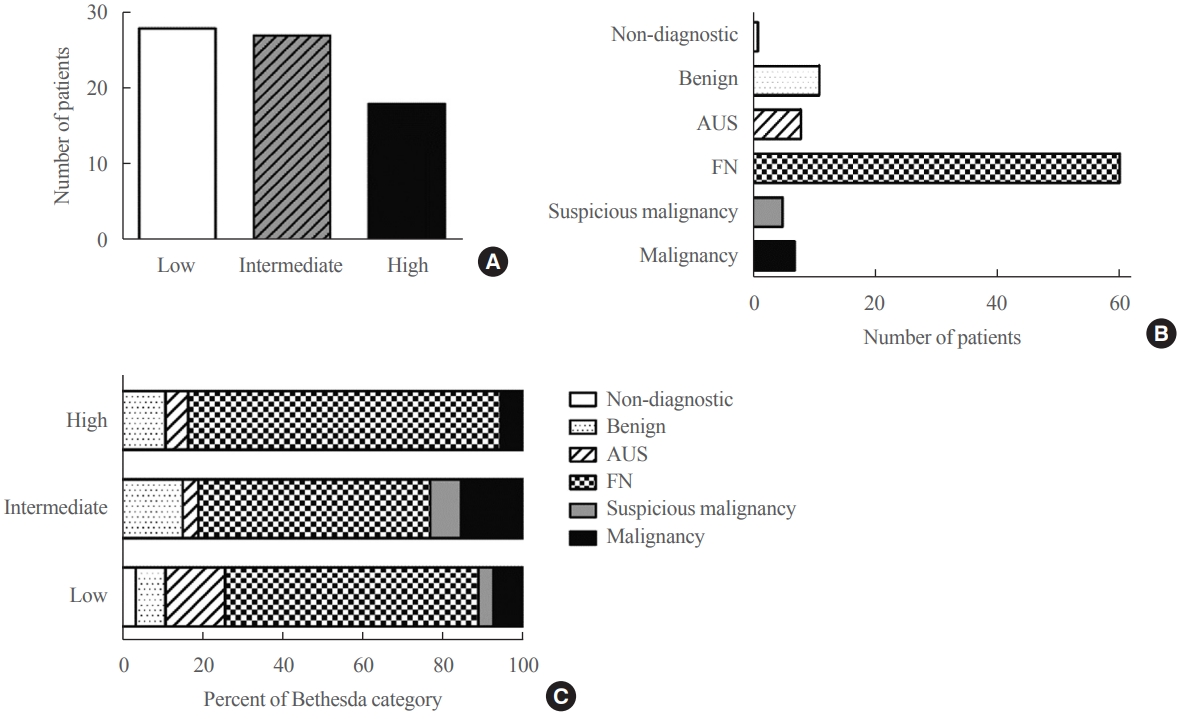
The mean age of the 97 patients included in the study was 50.3 years, and 26.8% were male. The mean size of the primary tumor was 3.2±1.8 cm, and three (3.1%) patients had distant metastasis at initial diagnosis. Ultrasonographic findings were available for 73 patients; the number of nodules with low-, intermediate-, and high suspicion was 28 (38.4%), 27 (37.0%), and 18 (24.7%), respectively, based on the Korean-Thyroid Imaging Reporting and Data System. Preoperatively, follicular neoplasm (FN) or suspicion for FN accounted for 65.2% of the cases according to the Bethesda category, and 13% had malignancy or suspicious for malignancy. During a median follow-up of 8.5 years, eight (8.2%) patients had persistent/recurrent disease, and none died of HCC. Older age, gross extrathyroidal extension (ETE), and widely invasive types of tumors were significantly associated with distant metastasis (all P<0.01). Gross ETE (hazard ratio [HR], 27.7; 95% confidence interval [CI], 2.2 to 346.4; P=0.01) and widely invasive classification (HR, 6.5; 95% CI, 1.1 to 39.4; P=0.04) were independent risk factors for poor disease-free survival (DFS).
Conclusion
The long-term prognosis of HCC is relatively favorable in South Korea from this study, although this is not a nation-wide data, and gross ETE and widely invasive cancer are significant prognostic factors for DFS. The diagnosis of HCC by ultrasonography and cytopathology remains challenging. -
Citations
Citations to this article as recorded by- Molecular Alterations and Comprehensive Clinical Management of Oncocytic Thyroid Carcinoma
Lindsay A. Bischoff, Ian Ganly, Laura Fugazzola, Erin Buczek, William C. Faquin, Bryan R. Haugen, Bryan McIver, Caitlin P. McMullen, Kate Newbold, Daniel J. Rocke, Marika D. Russell, Mabel Ryder, Peter M. Sadow, Eric Sherman, Maisie Shindo, David C. Shonk
JAMA Otolaryngology–Head & Neck Surgery.2024; 150(3): 265. CrossRef - Oncocytic carcinoma of the thyroid: Conclusions from a 20‐year patient cohort
Nelson R. Gruszczynski, Shahzeb S. Hasan, Ana G. Brennan, Julian De La Chapa, Adithya S. Reddy, David N. Martin, Prem P. Batchala, Edward B. Stelow, Eric M. Dowling, Katherine L. Fedder, Jonathan C. Garneau, David C. Shonka
Head & Neck.2024;[Epub] CrossRef - Hurthle cell carcinoma: a rare variant of thyroid malignancy – a case report
Yuvraj Adhikari, Anupama Marasini, Nawaraj Adhikari, Laxman D. Paneru, Binit Upadhaya Regmi, Manita Raut
Annals of Medicine & Surgery.2023; 85(5): 1940. CrossRef - Hürthle Cell Carcinoma: Single Center Analysis and Considerations for Surgical Management Based on the Recent Literature
Costanza Chiapponi, Milan J.M. Hartmann, Matthias Schmidt, Michael Faust, Christiane J. Bruns, Anne M. Schultheis, Hakan Alakus
Frontiers in Endocrinology.2022;[Epub] CrossRef
- Molecular Alterations and Comprehensive Clinical Management of Oncocytic Thyroid Carcinoma
Image of Interest
- Thyroid
- Anaplastic Thyroid Carcinoma with Initial Ultrasonography Features Mimicking Subacute Thyroiditis
- Meihua Jin, Tae Yong Kim
- Endocrinol Metab. 2021;36(1):201-202. Published online February 24, 2021
- DOI: https://doi.org/10.3803/EnM.2020.884
- 3,283 View
- 133 Download
- 1 Web of Science
- 2 Crossref
-
PDFPubReader ePub
-
Citations
Citations to this article as recorded by- Ibuprofen inhibits anaplastic thyroid cells in vivo and in vitro by triggering NLRP3-ASC-GSDMD-dependent pyroptosis
Haohao Guo, Runsheng Ma, Yifei Zhang, Keyu Yin, Gongbo Du, Fanxiang Yin, Hongqiang Li, Ziyang Wang, Detao Yin
Inflammopharmacology.2024; 32(1): 733. CrossRef - The Old and the New in Subacute Thyroiditis: An Integrative Review
Nicola Lanzo, Bohdan Patera, Gaia Fazzino, Daniela Gallo, Adriana Lai, Eliana Piantanida, Silvia Ippolito, Maria Tanda
Endocrines.2022; 3(3): 391. CrossRef
- Ibuprofen inhibits anaplastic thyroid cells in vivo and in vitro by triggering NLRP3-ASC-GSDMD-dependent pyroptosis
Original Articles
- Clinical Study
- Clinical Outcomes after Early and Delayed Radioiodine Remnant Ablation in Patients with Low-Risk Papillary Thyroid Carcinoma: Propensity Score Matching Analysis
- Jonghwa Ahn, Meihua Jin, Eyun Song, Min Ji Jeon, Tae Yong Kim, Jin-Sook Ryu, Won Bae Kim, Young Kee Shong, Ji Min Han, Won Gu Kim
- Endocrinol Metab. 2020;35(4):830-837. Published online November 18, 2020
- DOI: https://doi.org/10.3803/EnM.2020.747

- 4,239 View
- 132 Download
- 3 Web of Science
- 6 Crossref
-
Abstract
PDFSupplementary MaterialPubReader ePub
- Background
The clinical outcomes of delayed radioiodine remnant ablation (RRA) therapy in patients with low-risk papillary thyroid carcinoma (PTC) are unclear. We aimed to evaluate the clinical impact of the interval between total thyroidectomy (TT) and RRA therapy in patients with low-risk PTC.
Methods
We included 526 patients who underwent TT and RRA for low-risk PTC with a primary tumor size of >1 cm between 2000 and 2012. Patients were divided into the early (<90 days) and the delayed (≥90 days) RRA groups based on the interval between TT and RRA. The results of diagnostic whole-body scan (DxWBS), ongoing risk stratification (ORS; response to therapy), and disease-free survival (DFS) were evaluated before and after propensity score matching (PSM).
Results
Among the 526 patients, 75 (14.3%) patients underwent delayed RRA; they had more cervical lymph node metastasis and received a higher RRA dose than those who underwent early RRA. The median follow-up period was 9.1 years after initial therapy, and the structural recurrence rate was 1.9%. In DxWBS, 60 patients had focal iodine uptake limited in operative bed, with no significant difference between groups. According to ORS, 78%, 20%, 1%, and 1% patients were classified into excellent, indeterminate, biochemical incomplete, and structural incomplete response groups, respectively. There was no significant difference in ORS or DFS between groups before and after PSM.
Conclusion
The timing of the first RRA had no clinical impact in patients with low-risk PTC. Thus, the clinical decision for RRA can be determined >3 months after TT considering other prognostic factors. -
Citations
Citations to this article as recorded by- Dynamic risk assessment in patients with differentiated thyroid cancer
Erika Abelleira, Fernando Jerkovich
Reviews in Endocrine and Metabolic Disorders.2024; 25(1): 79. CrossRef - Ablation Rates and Long-Term Outcome Following Low-Dose Radioiodine for Differentiated Thyroid Cancer in the West of Scotland: A Retrospective Analysis
Kathryn Graham, Fay Tough, Helena Belikova, Irene Wotherspoon, David Colville, Nicholas Reed
Endocrine Practice.2024; 30(4): 327. CrossRef - Radioiodine ablation after thyroidectomy could be safely abandoned or postponed in selected stage I papillary thyroid carcinoma patients of low-risk group: an observational prospective study
S.M. Cherenko, A.Yu. Glagolieva, D.E. Makhmudov
INTERNATIONAL JOURNAL OF ENDOCRINOLOGY (Ukraine).2024; 20(1): 7. CrossRef - Patient Preparation and Radiation Protection Guidance for Adult Patients Undergoing Radioiodine Treatment for Thyroid Cancer in the UK
J. Wadsley, N. Armstrong, V. Bassett-Smith, M. Beasley, R. Chandler, L. Cluny, A.J. Craig, K. Farnell, K. Garcez, N. Garnham, K. Graham, A. Hallam, S. Hill, H. Hobrough, F. McKiddie, M.W.J. Strachan
Clinical Oncology.2023; 35(1): 42. CrossRef - Delay of initial radioactive iodine therapy beyond 3 months has no effect on clinical responses and overall survival in patients with thyroid carcinoma: A cohort study and a meta‐analysis
Fang Cheng, Juan Xiao, Fengyan Huang, Chunchun Shao, Shouluan Ding, Canhua Yun, Hongying Jia
Cancer Medicine.2022; 11(12): 2386. CrossRef - Delayed (>3 Months) Postoperative Radioactive Iodine Ablation Does Not Impact Clinical Response or Survival in Differentiated Thyroid Cancers
Tatiana Fedorova, Lilah F. Morris-Wiseman
Clinical Thyroidology.2022; 34(10): 456. CrossRef
- Dynamic risk assessment in patients with differentiated thyroid cancer
- Clinical Study
- Clinical Implication of World Health Organization Classification in Patients with Follicular Thyroid Carcinoma in South Korea: A Multicenter Cohort Study
- Meihua Jin, Eun Sook Kim, Bo Hyun Kim, Hee Kyung Kim, Hyon-Seung Yi, Min Ji Jeon, Tae Yong Kim, Ho-Cheol Kang, Won Bae Kim, Young Kee Shong, Mijin Kim, Won Gu Kim
- Endocrinol Metab. 2020;35(3):618-627. Published online September 22, 2020
- DOI: https://doi.org/10.3803/EnM.2020.742
- 5,414 View
- 121 Download
- 8 Web of Science
- 9 Crossref
-
Abstract
PDFPubReader ePub
- Background
The study aimed to compare the prognostic value of the 4th edition of World Health Organization classification (WHO-2017) with the previous WHO classification (WHO-2004) for follicular thyroid carcinoma (FTC).
Methods
This multicenter retrospective cohort study included 318 patients with FTC from five tertiary centers who underwent thyroid surgery between 1996 and 2009. We evaluated the prognosis of patients with minimally invasive (MI), encapsulated angioinvasive (EA), and widely invasive (WI) FTC according to WHO-2017. Further, we evaluated the proportion of variation explained (PVE) and Harrell’s C-index to compare the predictability of disease-free survival (DFS) and disease-specific survival (DSS).
Results
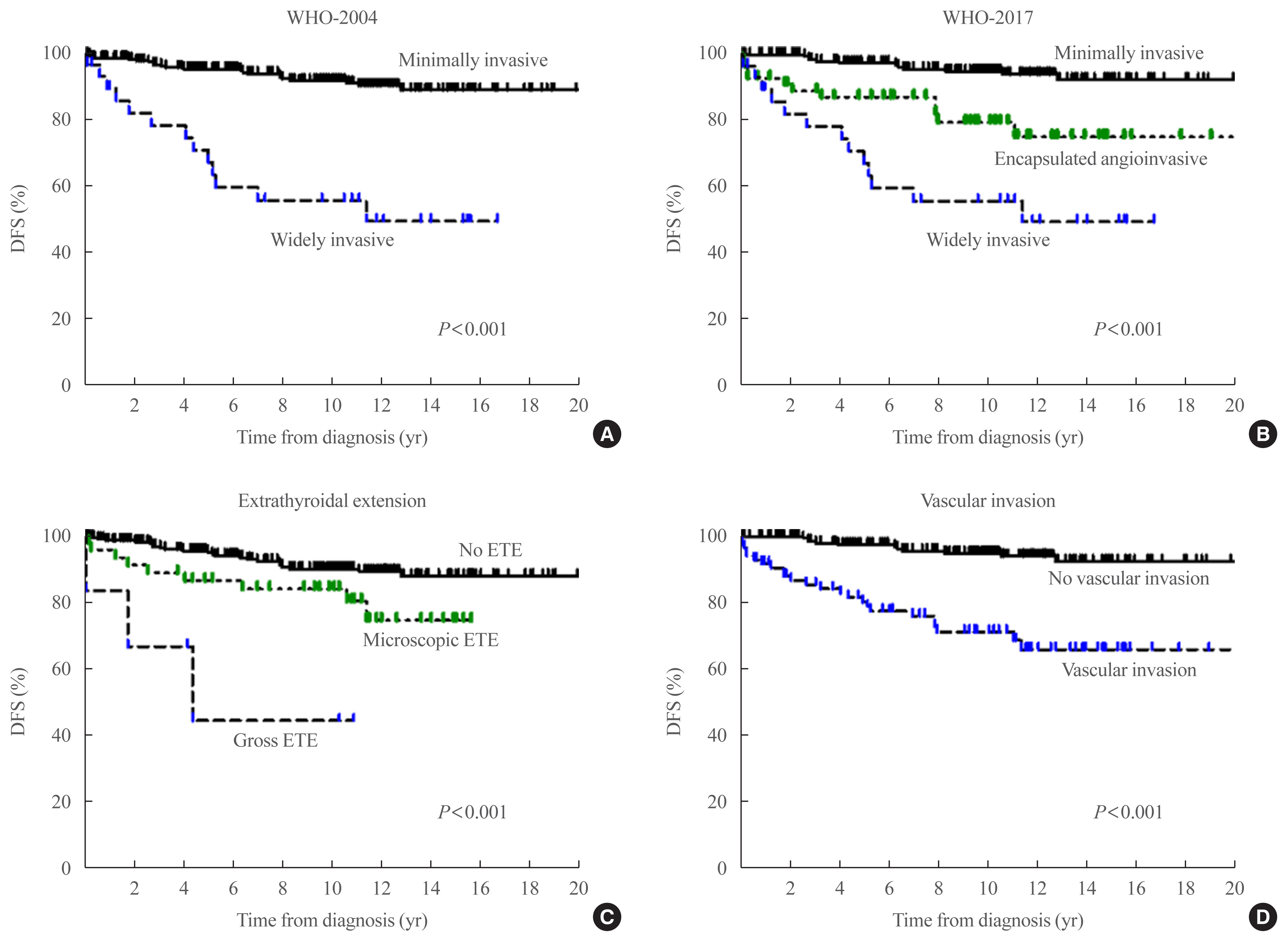
In total, 227, 58, and 33 patients had MI-, EA-, and WI-FTC, respectively. During a median follow-up of 10.6 years, 46 (14.5%) patients had disease recurrence and 20 (6.3%) patients died from FTC. The 10-year DFS rates of patients with MI-, EA-, and WI-FTC were 91.1%, 78.2%, and 54.9%, respectively (P<0.001, PVE=7.1%, C-index=0.649). The corresponding 10-year DSS rates were 95.9%, 93.5%, and 73.5%, respectively (P<0.001, PVE=2.6%, C-index=0.624). The PVE and C-index values were higher using WHO-2017 than using WHO-2004 for the prediction of DFS, but not for DSS. In multivariate analysis, older age (P=0.02), gross extrathyroidal extension (ETE) (P=0.003), and distant metastasis (P<0.001) were independent risk factors for DSS.
Conclusion
WHO-2017 improves the predictability of DFS, but not DSS, in patients with FTC. Distant metastasis, gross ETE and older age (≥55 years) were independent risk factors for DSS. -
Citations
Citations to this article as recorded by- Association of Ultrasonography Features of Follicular Thyroid Carcinoma With Tumor Invasiveness and Prognosis Based on WHO Classification and TERT Promoter Mutation
Myoung Kyoung Kim, Hyunju Park, Young Lyun Oh, Jung Hee Shin, Tae Hyuk Kim, Soo Yeon Hahn
Korean Journal of Radiology.2024; 25(1): 103. CrossRef - Clinical Outcomes and Implications of Radioactive Iodine Therapy on Cancer-specific Survival in WHO Classification of FTC
Genpeng Li, Ziyang Ye, Tao Wei, Jingqiang Zhu, Zhihui Li, Jianyong Lei
The Journal of Clinical Endocrinology & Metabolism.2024;[Epub] CrossRef - Radioiodine whole body scan pitfalls in differentiated thyroid cancer
Cristina Basso, Alessandra Colapinto, Valentina Vicennati, Alessandra Gambineri, Carla Pelusi, Guido Di Dalmazi, Elisa Lodi Rizzini, Elena Tabacchi, Arber Golemi, Letizia Calderoni, Stefano Fanti, Uberto Pagotto, Andrea Repaci
Endocrine.2024;[Epub] CrossRef - The Prognostic Impact of Extent of Vascular Invasion in Follicular Thyroid Carcinoma
David Leong, Anthony J. Gill, John Turchini, Michael Waller, Roderick Clifton‐Bligh, Anthony Glover, Mark Sywak, Stan Sidhu
World Journal of Surgery.2023; 47(2): 412. CrossRef - TERT Promoter Mutation as a Prognostic Marker in Encapsulated Angioinvasive and Widely Invasive Follicular Thyroid Carcinomas
Yasuhiro Ito, Takashi Akamizu
Clinical Thyroidology.2023; 35(5): 202. CrossRef - Risk factors for death of follicular thyroid carcinoma: a systematic review and meta-analysis
Ting Zhang, Liang He, Zhihong Wang, Wenwu Dong, Wei Sun, Ping Zhang, Hao Zhang
Endocrine.2023; 82(3): 457. CrossRef - Molecular classification of follicular thyroid carcinoma based on TERT promoter mutations
Hyunju Park, Hyeong Chan Shin, Heera Yang, Jung Heo, Chang-Seok Ki, Hye Seung Kim, Jung-Han Kim, Soo Yeon Hahn, Yun Jae Chung, Sun Wook Kim, Jae Hoon Chung, Young Lyun Oh, Tae Hyuk Kim
Modern Pathology.2022; 35(2): 186. CrossRef - Whole-genome Sequencing of Follicular Thyroid Carcinomas Reveal Recurrent Mutations in MicroRNA Processing Subunit DGCR8
Johan O Paulsson, Nima Rafati, Sebastian DiLorenzo, Yi Chen, Felix Haglund, Jan Zedenius, C Christofer Juhlin
The Journal of Clinical Endocrinology & Metabolism.2021; 106(11): 3265. CrossRef - Clinicopathological Characteristics and Disease-Free Survival in Patients with Hürthle Cell Carcinoma: A Multicenter Cohort Study in South Korea
Meihua Jin, Eun Sook Kim, Bo Hyun Kim, Hee Kyung Kim, Yea Eun Kang, Min Ji Jeon, Tae Yong Kim, Ho-Cheol Kang, Won Bae Kim, Young Kee Shong, Mijin Kim, Won Gu Kim
Endocrinology and Metabolism.2021; 36(5): 1078. CrossRef
- Association of Ultrasonography Features of Follicular Thyroid Carcinoma With Tumor Invasiveness and Prognosis Based on WHO Classification and TERT Promoter Mutation
- Clinical Study
- Clinical Outcomes of N1b Papillary Thyroid Cancer Patients Treated with Two Different Doses of Radioiodine Ablation Therapy
- Meihua Jin, Jonghwa Ahn, Yu-Mi Lee, Tae-Yon Sung, Won Gu Kim, Tae Yong Kim, Jin-Sook Ryu, Won Bae Kim, Young Kee Shong, Min Ji Jeon
- Endocrinol Metab. 2020;35(3):602-609. Published online September 22, 2020
- DOI: https://doi.org/10.3803/EnM.2020.741
- 5,401 View
- 121 Download
- 1 Web of Science
-
Abstract
PDFPubReader ePub
- Background
The optimal dose of radioactive iodine (RAI) therapy for N1b papillary thyroid carcinoma (PTC) is controversial. We evaluated the clinical outcome of N1b PTC patients treated with either 100 or 150 mCi of RAI.
Methods
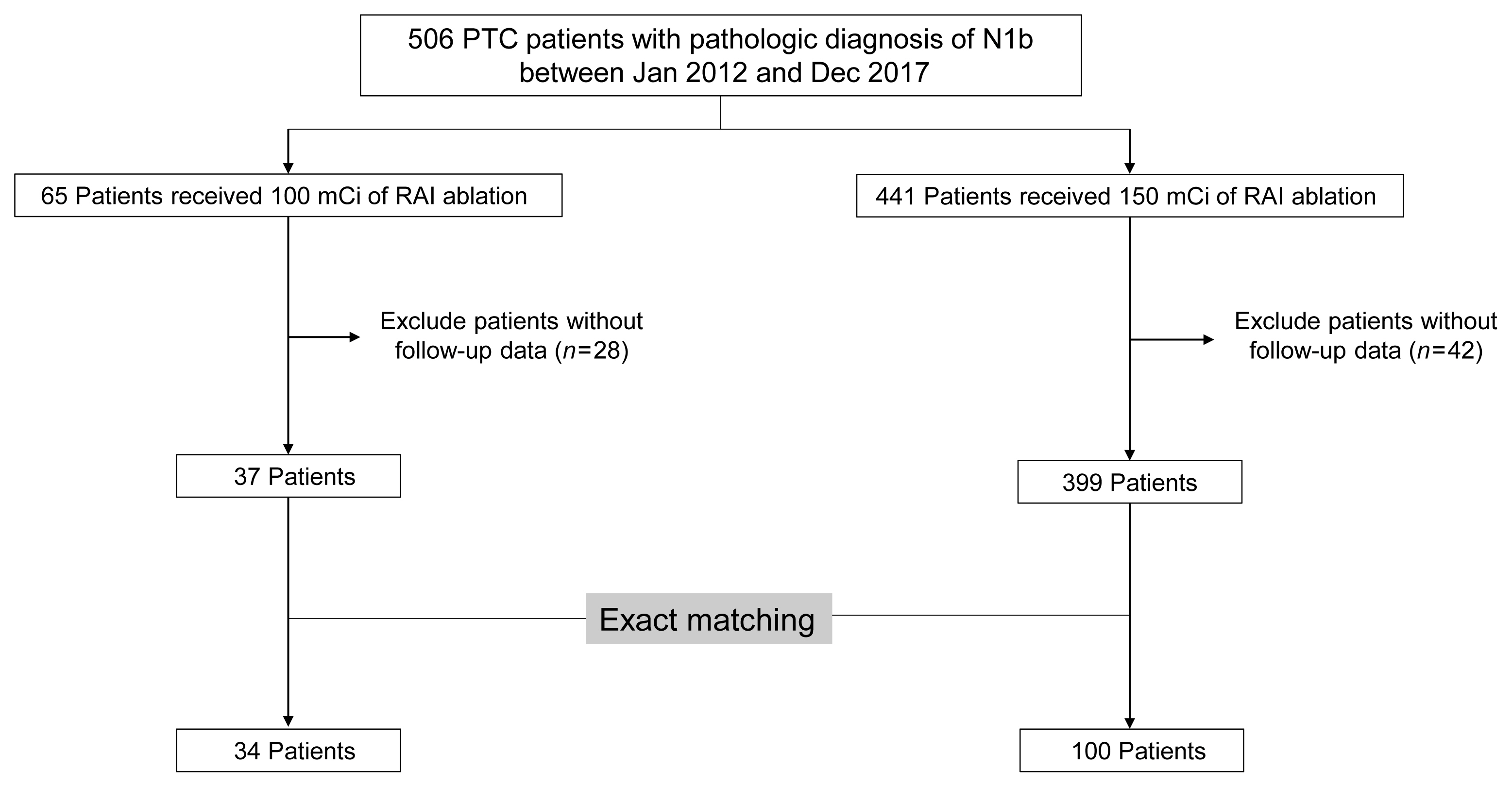
We retrospectively analyzed N1b PTC patients who underwent total thyroidectomy and postoperative RAI therapy at a tertiary referral center between 2012 and 2017. As the baseline characteristics differed between treatment groups, we performed exact matching for various pathological factors according to RAI dose. We evaluated the response to therapy and recurrence-free survival (RFS) in the matched patients. Structural recurrent/persistent disease was defined as new structural disease detected after initial therapy, which was confirmed by cytology or pathology.
Results
Of the total 436 patients, 37 (8.5%) received 100 mCi of RAI and 399 (91.5%) received 150 mCi of RAI. After an exact 1:3 matching, 34 patients in the 100 mCi group and 100 patients in the 150 mCi group remained. There was no significant difference in response to therapy between the groups in the matched population (P=0.63). An excellent response was achieved in 70.6% (n=24) of patients in the 100 mCi group and 76.0% (n=76) in the 150 mCi group. Two (5.9%) patients in the 100 mCi group and four (4.0%) in the 150 mCi group had recurrence and there was no significant difference in RFS between the groups in the matched population (P=0.351).
Conclusion
There were no differences in response to therapy and RFS in N1b PTC patients according to RAI dose.
 First
First Prev
Prev


